Nutritional Deficiency: Symptoms, Causes, and Treatment
- Alvi Moreno
- 2 days ago
- 8 min read

TL;DR:
Nutritional deficiencies occur when the body lacks sufficient essential vitamins or minerals needed for normal function, leading to health problems such as fatigue, anemia, and neurological damage. Diagnosis involves clinical history, risk assessment, and blood tests, with functional biomarkers like EGRac and MMA providing more reliable evidence than symptoms alone. Treatment varies from dietary modifications and oral supplements to injections, depending on the cause, with early detection being key to effective management.
A nutritional deficiency is defined as a state in which the body lacks adequate amounts of one or more essential vitamins or minerals required for normal physiological function. According to Healthdirect and Penn Medicine, this shortfall triggers a cascade of health problems ranging from fatigue and anemia to irreversible neurological damage. The root causes split into three categories: insufficient dietary intake, poor absorption, and elevated physiological demand. Each category requires a different fix, which is why understanding the type of deficiency you are dealing with matters as much as identifying it in the first place. This article covers the most common deficiencies, how they are diagnosed, what drives them, and how to treat them effectively.
What are the most common nutritional deficiencies and their symptoms?
Iron deficiency is the most widespread nutritional deficiency globally, and its primary presentation is anemia. Symptoms include persistent fatigue, pallor, shortness of breath, and reduced concentration. Many people attribute these signs to stress or poor sleep, which delays diagnosis by months. The symptoms vary widely depending on severity, and untreated cases can cause lasting organ damage.
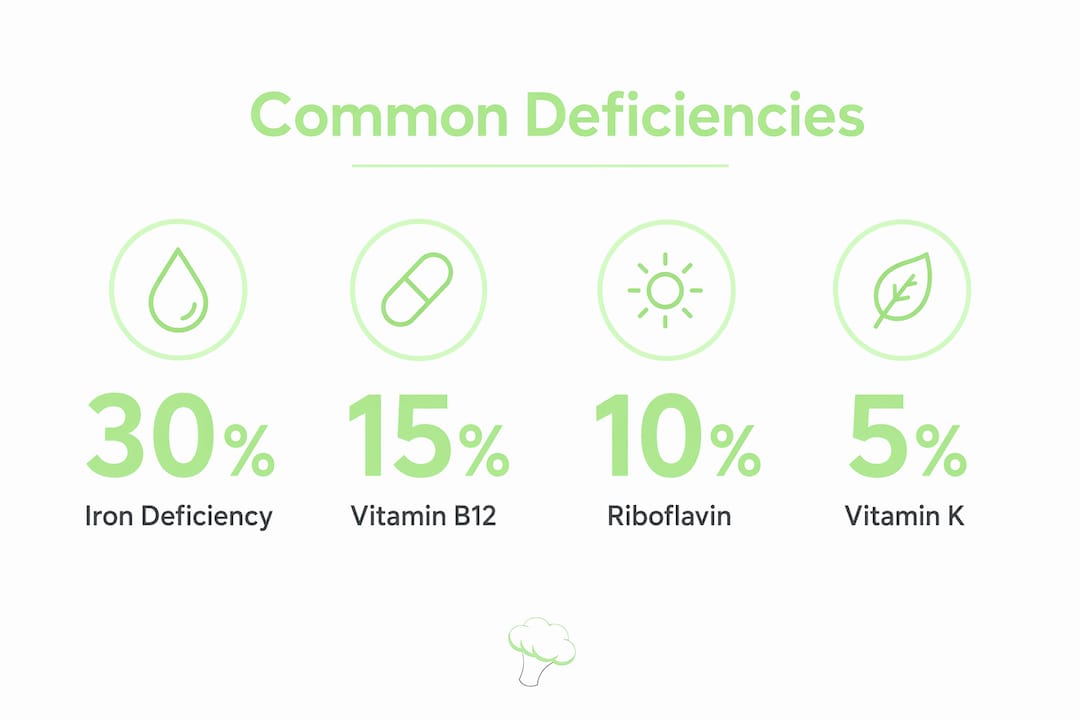
Vitamin B12 deficiency produces a distinct symptom profile that overlaps with neurological disease. You may notice tingling in the hands and feet, memory problems, mood changes, and a smooth, inflamed tongue. Megaloblastic anemia, where red blood cells grow abnormally large, is the hallmark lab finding. Because B12 is stored in the liver for years, symptoms often appear long after dietary intake has dropped.
Riboflavin (vitamin B2) deficiency causes mucocutaneous lesions, meaning sores at the corners of the mouth, a swollen magenta-colored tongue, and skin rashes around the nose and genitals. It also contributes to normochromic anemia and frequently co-occurs with other B-vitamin deficiencies. This makes it easy to miss as a standalone diagnosis.
Vitamin D deficiency affects bone metabolism and immune regulation. In children, severe deficiency causes rickets, a condition marked by soft, deformed bones. Adults develop osteomalacia, presenting as bone pain and muscle weakness. Because vitamin D is synthesized through sun exposure, people in northern latitudes or those who spend most of their time indoors carry the highest risk.
Key symptoms to watch across deficiency types:
Iron: Fatigue, pallor, brittle nails, cold hands and feet
Vitamin B12: Tingling limbs, memory lapses, megaloblastic anemia
Riboflavin: Mouth sores, inflamed tongue, skin lesions
Vitamin D: Bone pain, muscle weakness, frequent infections
Vitamin K: Easy bruising, prolonged bleeding from cuts, heavy menstrual periods
Vitamin K deficiency is rare in healthy adults but serious in newborns, where it causes vitamin K deficiency bleeding. Standard prevention is a 1 mg intramuscular injection at birth, which is more reliable than oral methods. This is one of the few deficiencies where a single clinical intervention at a predictable moment eliminates most risk.
How are nutritional deficiencies diagnosed and assessed?
Diagnosis starts with clinical history and a structured risk factor evaluation. A clinician will ask about diet patterns, medications, recent surgeries, alcohol use, and symptoms. This step narrows the list of likely deficiencies before any blood is drawn. Skipping this step and going straight to labs often produces results that are hard to interpret without context.
Blood tests are the primary diagnostic tool. The most commonly ordered panels include:
Hemoglobin and hematocrit for anemia screening
Serum ferritin and iron indices for iron status
Serum B12 and methylmalonic acid (MMA) for B12 deficiency
Erythrocyte glutathione reductase activation coefficient (EGRac) for riboflavin
25-hydroxyvitamin D for vitamin D status
Prothrombin time (PT) for vitamin K function
EGRac above 1.4 is the accepted cutoff for diagnosing riboflavin deficiency, and it is considered more reliable than serum riboflavin alone. This matters because serum levels fluctuate with recent food intake, while EGRac reflects functional enzyme activity over time. For a detailed breakdown of nutrient types and their deficiency signs, the nutrient deficiency guide on Bimiapp covers each micronutrient systematically.
One critical nuance: inflammation elevates ferritin as an acute-phase reactant, which can mask true iron deficiency. A patient with active infection or chronic inflammatory disease may show a normal or even high ferritin reading despite being genuinely iron depleted. Clinicians address this by combining ferritin with transferrin saturation, soluble transferrin receptor levels, and clinical history.
Nutrient | Primary Test | Key Cutoff or Marker |
Iron | Serum ferritin, transferrin saturation | Ferritin below 12 mcg/L (uncomplicated) |
Vitamin B12 | Serum B12, methylmalonic acid | MMA elevation confirms functional deficiency |
Riboflavin | EGRac | EGRac above 1.4 |
Vitamin D | 25-hydroxyvitamin D | Below 20 ng/mL indicates deficiency |
Vitamin K | Prothrombin time | Prolonged PT suggests functional deficiency |
Pro Tip: Fast for at least 8 hours before iron and B12 panels. Recent meals can temporarily raise serum B12 and alter iron indices, producing falsely reassuring results.
What causes nutritional deficiencies and who is most at risk?
Deficiencies divide into two mechanistic categories. Primary deficiency results from insufficient dietary intake. Secondary deficiency occurs when intake is adequate but absorption, metabolism, or excretion is disrupted. Distinguishing between the two is the first step toward effective treatment, because the same supplement dose that corrects a dietary gap will fail completely in a malabsorption case.

Dietary causes are straightforward but often underestimated. Strict vegan diets eliminate all animal-sourced B12, making supplementation non-negotiable for that population. Highly processed food patterns displace nutrient-dense whole foods, creating multiple simultaneous gaps. Calorie-restricted diets, even well-intentioned ones, frequently fall short on iron, zinc, and riboflavin.
Medical and physiological causes are more complex:
Celiac disease and Crohn’s disease damage the intestinal lining, reducing absorption of iron, B12, and fat-soluble vitamins
Gastric bypass surgery removes the section of the stomach that produces intrinsic factor, making B12 absorption impossible without injections
Chronic blood loss from heavy menstruation or gastrointestinal bleeding depletes iron faster than diet can replace it
Alcohol use disorder impairs absorption and metabolism of thiamine, folate, and B12 simultaneously
Pregnancy and lactation increase demand for folate, iron, iodine, and vitamin D beyond what most diets provide
Populations with elevated risk include children during rapid growth phases, adults over 65 (who produce less stomach acid and absorb B12 less efficiently), individuals following restrictive diets, and anyone with a chronic gastrointestinal condition. The micronutrient deficiency guide on Bimiapp maps these risk factors to specific nutrients, which helps you prioritize where to focus your tracking.
How can dietary deficiencies be effectively treated and managed?
Treatment follows the cause. Oral supplementation works well for primary, intake-related deficiencies. Malabsorption cases require alternative delivery routes. Here is a practical framework for the most common deficiencies:
Iron deficiency anemia. Start with oral ferrous sulfate or ferrous gluconate, typically 150 to 200 mg of elemental iron per day in divided doses. Hemoglobin rises by at least 1 g/dL within 2 to 4 weeks of starting treatment in a responsive patient. Full repletion of iron stores takes 3 to 6 months. If hemoglobin does not rise as expected, suspect ongoing blood loss or non-adherence before increasing the dose.
Vitamin B12 deficiency. For dietary causes, high-dose oral B12 (1,000 mcg daily) corrects the deficiency reliably. Symptoms improve within days of starting treatment. For malabsorption, including pernicious anemia or post-gastric bypass cases, intramuscular injections every 1 to 3 months are required indefinitely, even after blood levels normalize.
Riboflavin deficiency. Oral riboflavin at 5 to 10 mg daily resolves most cases within weeks. Dietary sources include dairy products, eggs, lean meats, and fortified cereals. Because riboflavin deficiency rarely occurs in isolation, check for co-existing iron and B6 deficiencies.
Vitamin D deficiency. High-dose loading protocols (50,000 IU weekly for 8 to 12 weeks) correct deficiency, followed by maintenance doses of 1,500 to 2,000 IU daily. Recheck 25-hydroxyvitamin D levels after 3 months to confirm response.
Thiamine (B1) deficiency. Early parenteral thiamine is critical in high-risk patients, particularly those with alcohol use disorder or severe malnutrition. Neurological damage from thiamine deficiency is only partially reversible, making speed of treatment the single most important variable.
Pro Tip: Take iron supplements with vitamin C (ascorbic acid) to increase absorption by up to 67%. Avoid taking iron with calcium supplements, coffee, or tea, which all reduce absorption significantly.
Dietary optimization runs parallel to supplementation. Prioritize iron-rich foods like lean red meat, lentils, and fortified cereals. Add vitamin D through fatty fish and fortified dairy. For B12, focus on eggs, shellfish, and dairy if you eat animal products. Tracking your actual intake against your personal requirements is the most direct way to identify gaps before they become clinical problems.
Key takeaways
Nutritional deficiency requires identifying both the specific nutrient gap and its underlying cause before treatment can succeed.
Point | Details |
Define the deficiency type | Distinguish primary (low intake) from secondary (malabsorption) to choose the right treatment. |
Use functional biomarkers | Tests like EGRac and MMA confirm deficiency more reliably than symptoms or serum levels alone. |
Match treatment to cause | Oral supplements correct dietary gaps; injections are required when absorption is impaired. |
Monitor treatment response | Hemoglobin should rise within 2 to 4 weeks on iron therapy; B12 symptoms improve within days. |
Track intake proactively | Monitoring over 60 nutrients daily catches gaps before they produce clinical symptoms. |
What I have learned from watching deficiencies get missed
Most deficiencies I have seen go undetected for one reason: people wait for dramatic symptoms before acting. Fatigue gets blamed on work. Tingling fingers get dismissed as posture. By the time a lab result confirms what the body has been signaling for months, the deficiency is often entrenched and harder to reverse.
The other pattern I keep seeing is over-reliance on a single test. A normal serum B12 does not rule out functional B12 deficiency if methylmalonic acid is elevated. A normal ferritin in someone with active inflammation tells you almost nothing about true iron stores. The lab result only makes sense alongside the clinical picture.
What actually works is combining consistent intake tracking with periodic targeted testing. You do not need to test everything every month. You need to know which nutrients your diet consistently falls short on, and then confirm with labs when the pattern is clear. Whole-food sources should anchor your nutrition, with supplementation filling specific, confirmed gaps rather than acting as a blanket insurance policy. That approach is more sustainable, more precise, and far less likely to create new imbalances while correcting old ones.
— Alvi
Track your nutrients and catch deficiencies early with Bimiapp
Identifying a deficiency before it produces symptoms is the most effective form of management. Bimiapp monitors over 60 nutrients, including iron, B12, riboflavin, vitamin D, and vitamin K, giving you a precise daily picture of where your intake stands relative to your personal requirements.
The platform uses AI photo recognition to log meals in seconds, then maps your intake against targets calibrated to your age, weight, and activity level. You can spot a consistent riboflavin gap or a vitamin D shortfall weeks before any blood test would flag it. See how Bimiapp works and start tracking the nutrients that matter most to your health.
FAQ
What is a nutritional deficiency?
A nutritional deficiency occurs when the body does not receive or absorb enough of a specific vitamin or mineral to maintain normal function. It can result from low dietary intake, poor absorption, or increased physiological demand.
What are the most common symptoms of deficiency?
Symptoms depend on the nutrient involved but commonly include fatigue, anemia, bone pain, neurological changes, and skin or mucosal lesions. Iron deficiency causes pallor and exhaustion, while B12 deficiency produces tingling and memory problems.
How is a vitamin deficiency diagnosed?
Diagnosis combines clinical history with blood tests such as serum ferritin, B12, methylmalonic acid, EGRac for riboflavin, and 25-hydroxyvitamin D. Functional biomarkers provide more reliable evidence than symptoms alone.
How do you treat a nutritional deficiency?
Treatment depends on the cause. Dietary deficiencies respond to oral supplements and food-based corrections. Malabsorption cases, such as B12 deficiency after gastric bypass, require intramuscular injections. Most deficiencies show measurable improvement within 2 to 4 weeks of correct treatment.
Which groups are most at risk for nutrient deficiencies?
Children, pregnant women, adults over 65, people following restrictive diets, and individuals with gastrointestinal conditions like celiac disease or Crohn’s disease carry the highest risk. Review common risk groups to identify where your own risk profile sits.
Recommended
Comments